Chapter 5
Total Quality Management (TQM) Implementation and Impact Assesment in Healthcare: A Comprehensive Analysis
- Geetha Joshi (Assistant Professor Dayananda Sagar Business School, Bangalore)
- ISBN
- 978-81-963834-1-1
- Published
- 11 July 2026
- Accesses
- 8 views · 1 downloads
- Reading time
- ~32 min
Abstract
This qualitative research sought to understand and answer TQM's issues in healthcare. Service quality issues and TQM implementation hurdles are examined. Methodology/Approach: TQM implementation challenges investigated using a conceptual model. TQM has three primary components: implementation hurdles, Critical Success Factors, and benefits. Health care providers and patients were questioned using questionnaires. Seven hypotheses were created to evaluate how TQM may be achieved regardless of impediments. Findings: TQM can improve SQ, customer satisfaction, employee loyalty, profitability, and shareholder value in the right setting with dedicated leadership and enabling infrastructure. For industrial performance, TQM can deliver high-quality medical care. Limitations and Implications: Semi-structured research questionnaires were used during interviews. Review and questionnaire biases may exist. Originality and paper value:The research benefits from medical staff and patients' viewpoints on SQ features such quality circle, continuous improvement, employee empowerment, and customer-focused approach.
Keywords: Total Service Quality, Healthcare, Organisational Excellence, Perceived Satisfaction, And Operational Eficiency
Full text
Introduction
The manufacturing sector developed Total Quality Management (TQM) to assess plant and industry performance. TQM improves company performance by deliv-ering quality goods, services, and operations and maintenance. Quality manage-ment systems continuously modify processes to maximise customer satisfaction at the lowest cost, according to Zgodavova and Colesca (2007). Business benefits from improved service quality (SQ). SQ is crucial to the success of a product or service. Without it, it would fail. This may be quantified by comparing custom-ers’ quality expectations to what they actually receive—a service gap. (2015) Izo-go and Ogba Consumer loyalty is hampered by the service difference. Rework and unhappy customers make low-quality goods and services more costly than high-quality ones. SQ and TQM are crucial to every sector or corporation, regard-less of its nature.
TQM deployment enhanced corporate operations, according to Hassan et al. (2012). To offer a better product or service on the first attempt and consistently, TQM should be incorporated into the company culture. TQM enhances accom-plishment via a continuum of relevant attribute metrics throughout the value ad-dition spectrum. It helps make better goods that surpass customer expectations (Yusof and Aspinwall, 2001). Thus, TQM-implemented companies improved oper-ational efficiency, throughput, sales, revenue, and effectiveness.
Devoted leadership, a strong corporate culture, active engagement, and worker cohesion are key to TQM success. Leadership, collaboration, people management, and service delivery system are essential for TQM performance (Dahlgaard, Pet-tersen, and Park, 2011). Product and service production and delivery will be ap-propriately priced. TQM was first limited to the production line, but as time went on, it was concluded that the service sector should also comply with it, thus it was given a corresponding position in the service industry. According to Prajogoa and Hong (2008), TQM may create a suitable atmosphere outside of production or manufacturing. Quality must be promoted by high management.
Objectives
This research examines how technology, TQM axioms, practises, and pandem-ic implications affect the bottom line. The disaster has shown several countries’ healthcare systems’ shocking weaknesses and shortcomings. It has demanded a complete reevaluation of the nation’s healthcare infrastructure and the creation of a proper policy and plan to prevent repeat calamities. Even in a natural ca-tastrophe, healthcare services must be robust, according to Kajihara et al. (2016). Integrating the health policy with an adequate TQM policy creates a complete, efficient, and effective system. Therefore, these research goals have been set:
To Determine technology’s role in healthcare excellence.
To Assess TQM implementation in healthcare.
To examine TQM’s impact on profitability.
Concerns
This research examines TQM’s standing in the healthcare business, its shortcom-ings, problems, and implementation. The goal is to increase patients’ opinions of service providers based on their healthcare competency and quality care en-dowment. Based on a review of the literature and critical success factors (CSFs) like technology, quality compliance, team structure, customer-focused approach, and employee training and development, this study investigated the following research questions (RQs) and proposed corrective actions for implementing TQM practises in the healthcare sector:
Would technology help TQM? How well does TQM work?
How do patients evaluate healthcare practitioners’ CSFs?
How do TQM, quality care, and profit relate?
SQ was the CSF’s priority to boost customer satisfaction and income. A thorough investigation and understanding of key success elements. Thus, the current re-search is expected to improve TQM implementation tactics in healthcare. In this sense, a TQM framework closely integrated with the right healthcare policy frame-work would safeguard and preserve society and build a healthy, joyous country. Healthcare professionals, hospital executives, and health advocates will benefit from this concept. Methods, analysis, literature review, and conclusions follow.
Literature Review
Businesses must overcome several difficulties to adopt and execute TQM since it’s not a fast cure. Without leadership backing, TQM advantages seldom materialise. Industry, research, and academia are interested in it. In healthcare, TQM means focused efforts to enhance patient care, system performance, and profession-al growth. TQM and hospital success are linked, according to Ali and Alolayyan (2013). To improve healthcare, it involves changing clinical or administrative meth-ods or support. Healthcare taxonomy, SQ improvement, and TQM implementa-tion are discussed here.
Quality Service
Before addressing TQM, one must understand quality. Concerns include “Are we doing the right thing?” and “Are we doing things correctly?” Quality processes handle these two main issues in every area. The SERVQUAL idea by Parasura-man, Zeithaml, and Berry (1985) helps us grasp quality’s fluidity. It simply and successfully reflects customers’ expectations and views of a service. It claims that a customer’s SQ assessment causes the discrepancies between their expec-tations, evaluations, and actual performance. Parasuraman, Zeithaml, and Berry (1985), Parasuraman and Grewal (2000), and Parasuraman (2010) have published SERVQUAL applications. It was reduced from 10 components to five: Reliability, Assurance, Tangibles, Empathy, and Responsiveness (RATER). Various studies have
defined quality as:
Quality and customer pleasure (Kaoru Ishikawa, 1985).
Quality must be determined by the customer (Edwards Deming, 1986).
Joseph Juran (1989) defined quality as usability.
Oakland (2003) defines quality as customer satisfaction.
Although addressing end customers’ expectations and wants, the “common de-nominator” of these justifications. Based on their viewpoint and expertise, quality experts define quality differently. SQ is formed by customers’ perceptions and expectations, according to Parasuraman, Zeithaml, and Berry (1985). Improved SQ will enhance output and temporarily raise operational expenses. Thus, a manage-ment must decide how much to spend in quality to maximise return on quality. The return on quality technique allows executives to spend based on expected financial advantages such earnings and return on investments, according to Rust, Zahorik, and Keiningham (1995). Thus, client expectations and service provider performance may be compared to determine service excellence or lack thereof. Therefore, service providers must benchmark and assess the gap between cus-tomer expectations and actual delivery and how to reduce it. A CSF incorporates technology, team structures, a customer-focused strategy, senior management’s commitment to quality compliance, staff training, and quality planning, according to Deros, Yusof, and Salleh (2006). Calibrate operations and procedures using these. Given SQ’s importance and need, TQM and its effects are worth discussing. The following section discusses TQM subjects.
Quality Management
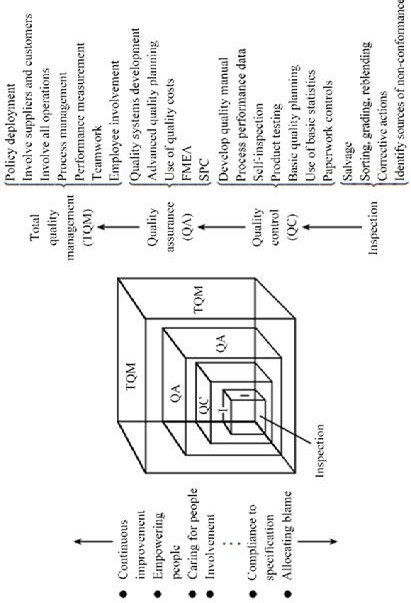
TQM was introduced in the early 1990s by Kaoru Ishikawa (1985), Edwards Deming (1986), Joseph Juran (1989), Hackman and Wageman (1995), and Oakland (2003). TQM has been characterised as “a search for excellence,” “perfection, first time and every time,” “zero defects,” “delighting the customer,” and more. Through continuous improvement (CI), innovation, waste reduction, improved productivity, increased sales, revenue, and profitability, the goal was to enhance customer hap-piness, staff satisfaction, and product and service quality. TQM implementation and acceptance will boost administrative performance, according to Hassan et al. (2012). Statistical process control is deeply ingrained in TQM. “Walter Shewhart” invented it in the early 1920s in the US. The technique categorised factors and found measurement anomalies in the manufacturing process. It produced a ra-tional manufacturing quality improvement method based on the PDCA (Plan-Do-Check-Act) mindset (Evans and Lindsay, 2001). TQM grew throughout time, and researchers discovered best practises. Figure 1 shows Dale, Wiele, and Iwaarden (2013)’s TQM evolution: Quality Enhancement, Quality Control (QC), Quality As-surance, and TQM.
Regardless of the business type, such as operation, production, healthcare service, hotel, consulting, or financial services, quality improvement and continuous im-provement remain indispensable business strategies. The successful organisation will never be satisfied with the status quo and will strive for CI of SQ to accomplish
TQM and progress towards Six Sigma. According to Antony et al. (2018), there are numerous growth opportunities for the implementation of SQ in healthcare. For their sustained success, prosperous businesses would seek out new ways to improve the quality of their products and SQ.
Rahman (2019) has identified seven best practises for TQM implementation based on a review of the relevant literature: leadership commitment, cooperation and collaboration, guidance, procedures, progressive growth, skill enhancement, and corporate philosophy. In addition, Rahman emphasised that these laws were ac-knowledged based on their phenomena and suggested that these implementa-tions have significant value in the healthcare industry. However, the definition of healthcare quality can vary based on the number of healthcare providers, the num-ber of patients, and the healthcare stakeholders involved in achieving SERVQUAL. Balasubramanian (2016) asserts that the SERVQUAL model and its application can aid healthcare in attaining service provider and consumer satisfaction, and that TQM can also be of great assistance to healthcare organisations.
TQM within the Health Care Industry
Healthcare services must satisfy the probability of intended outcomes and pro-duce the desired results in accordance with the organization’s preferences and expectations. Individual preferences, such as a customer-friendly environment, location, and even ambiance, may play a larger role in patients’ eventual satis-faction than adherence to standards and scientific evidence, clinical and ethical practises. According to Fatima, Malik, and Shabbir (2018), patient loyalty is pos-itively correlated with aspects of healthcare SQ such as natural ecosystem, con-sumer-friendly approach, attitude, confidentiality, and security.
Clinical and non-clinical services, procedures, and activities performed in response to issues such as “act virtuously” and “Implementing Things Right” constitute the core of healthcare. “Doing Right Things” evaluates the effectiveness of clinical service, whereas “Implementing Things Right” focuses on the methodological as-pects of healthcare service. Producing or being capable of producing a result would depend on how an organisation establishes and implements its procedures and processes, which would necessitate the guidance and support of manag-ers. According to Mosadeghrad (2013), the manager’s ability to adhere to TQM’s concepts and principles has a substantial effect on TQM’s implementation and influence. Effectiveness is the production of a desired outcome or output based on clinical knowledge and skills, whereas efficiency is the result of careful planning and execution. Avoiding the waste of materials, man hours, under-utilization of equipment, misuse of materials, energy, and amenities, and the failure to imple-ment correct ideas can increase efficiency. According to Dénes et al. (2017), inef-ficiency can lead to a lack of economies of scale and, as a result, increased costs. Care for patients and adherence to ethical principles should be given serious consideration for administrative effectiveness, employee welfare, and company profitability. According to Ansari (2020), SQ increases employee pride, and their efforts and motivation foster consumer loyalty and satisfaction, thereby promot-
ing recurrent purchase behaviour. Technical management or clinical performance will boost SQ, end-user loyalty, and customer satisfaction. Non- clinical adminis-tration, such as interpersonal skills, can facilitate patient care and co-production of services. The combination of clinical and nonclinical processes would eventually result in Total Quality Management. Ozdal and Oyebamiji (2018) state that TQM methods are implemented at all organisational levels, from the executive suite to the shop floor.
Research Methodology
On the basis of the research questions, research methods were developed. There-fore, qualitative research was conducted to investigate the research questions and strategies for overcoming the TQM framework’s challenges in the healthcare industry. Quantitative research was found to contribute the most, followed by blended and qualitative research. According to Cameron and Azorin (2011), quan-titative techniques account for 76% of research, making them the most popular method. Quantitative research accounts for 10%, while mixed methods account for 14%. Quantitative research was chosen to examine and extract the opinions, thoughts, and feelings of healthcare professionals and the general public regard-ing the significant impact of TQM attributes on the healthcare industry.
Consequently, the present researcher intended to conduct qualitative research by receiving direct feedback from medical professionals such as doctors, paramedics, and other supporting staff including clinical administrator, hospital administra-tion, medical records administrator, medical secretary, dieticians, and inpatients and outpatients. A common misconception is that sample size is irrelevant in qualitative research. Ultimately, determining an adequate sample size is a mat-ter of judgement that depends on a person’s skills in evaluating the quality of the collected data in relation to the sample size. However, various sample sizes have been proposed dependent on the topic of study. The sample size must be adequate to accomplish saturation and proportional to the research objectives. Therefore, adding additional participants beyond the saturation point will have no effect on the results.
The category of Phenomenology studies that investigate conscious experience,
i.e. subjective or first- person emotion. As Creswell (1998) suggests a sample size range of five to twenty-five for Phenomenology research, Morse (1994) recom-mended a minimum sample size of six for such investigations. Five samples were collected from physicians, paramedics, support staff, inpatients, and outpatients, respectively, based on sample significance and available literature recommenda-tions. Prior research samples were limited to healthcare professionals, and in some cases, patient feedback was obtained. In order to surmount the limitations of pre-vious research, this study considered an integrated chain of service employees. Utilising direct interviews with physicians, physiotherapists, nurses, technicians, supporting personnel, and patients, information about the integrated service chain was gathered. To notify professionals of the objective of the research and to finalise the interview schedule, an email was sent beforehand. The majority of
professionals requested that their interview not be recorded; as a result, conversa-tions are documented in writing. A few participants declined to participate, either because they were unfamiliar with the topic or because they did not wish to. Case-by-case, respondents were asked both structured and unstructured questions. According to Guetterman (2015), academics should address “how?” and “why?” before “how many?” when contemplating sample size. Participants were therefore asked pre-written questions. Patient feedback was collected after obtaining their permission, which was done randomly and without an appointment.
The interview script was developed through brainstorming and the formulation of straightforward, open-ended questions that enabled interviewees to do the ma-jority of the talking. The questionnaire was disseminated beforehand, giving the narrator time to prepare. In the beginning, fundamental questions were posed, in the middle, difficult and in-depth questions were posed, and in the end, clarifica-tions and expressions of gratitude were exchanged. The duration of the prepon-derance of interviews was between 30 and 40 minutes. Categorization of manually coded qualitative data involved determining the code frame, identifying the most prevalent theme, and subdividing into a hierarchical coding frame for locating relationships embedded with the responding emotion towards the topic.
Three System Model
As a result of developing the research model in accordance with the research ob-jectives and research questions, the system model was created. This system model represents the essence and spirit of a prototypical healthcare industry composed of multiple departmental elements, with SQ attributes serving as nodes and ar-rows serving as “causal” conduits connecting them. In particular, these paths ef-fectively connect and unify with TQM characteristics and are validated by analys-ing a cluster of hypotheses. The TQM conceptual framework, the verification of hypotheses, the findings, and the conclusion are depicted in Figure 2.
Total Quality Management (TQM) Implementation and Impact Assessment in Healthcare:
A Comprehensive Analysis | Githa Joshi
/ 9
H07
| TQM Main barrier | TQM key factors | TQM benefits |
|---|---|---|
| - Bureaucratic management - Lack of teamwork - Ineffective training | - Employee empowerment, customer focus - Quality Circle, Continuous improvement - Policies, processes, procedures, strategy, top management commitment | - Employee satisfaction & loyalty - Customer satisfaction and loyalty - Eliminating waste - Achievement of Lean manufacturing - Environmentally friendly system - Increased revenue and, profitability - Enhance shareholder value |
Examination of Hypotheses
The conceptual model demonstrating the important features of the current study is shown in Figure 2. It is divided into the parts Drivers, Benefits, CSFs, and Barriers. The crucial success factors (CSFs) of TQM, according to the model, are hindered by a number of issues. For producing these CSFs, the model shows a three-step, two-step, and three-branch process. The advantages that follow are produced by these CSFs. Three features link these two ends/segments viz. the appropri-ate mindset, professionalism, and consciousness. The “drivers” or “enablers” of TQM advantages are these CSFs. Through a review of the literature, Alzoubi et al. (2019), Antony et al. (2018), Balasubramanian (2016), Fatima, Malik, and Shabbir (2018), Mosadeghrad (2013), Ozdal and Oyebamiji (2018), and others developed questionnaires and hypotheses for a cross-sectional research. Seven hypotheses (H01-H07) were developed and assessed in the following paragraphs based on the conventional knowledge that already exists and involvement in service proj-ects and academic endeavours.
Increased company profitability is linked to TQM practices. Organisations must thus create a culture or environment that encourages and supports the use of TQM. The healthcare system faces challenges from a lack of administrative com-mitment, inexperienced middle-level management, and opposition to reform.
TQM is also significantly hampered by a lack of employee curiosity, inadequate skills, a lack of growth, and a lack of commitment, enthusiasm, and engagement on the side of the workforce. Additionally, medical personnel’ heavy workloads make it difficult for them to adopt the TQM culture. Sila and Ebrahimpour (2002) claim that problems with HRM, notably the establishment of a “iron curtain” be-tween divisions or functions, high staff turnover, and a “uncooperative” culture, are a barrier to achieving TQM. Employees frequently believe that TQM will bur-den them or compromise their “identity” because management finds it challeng-ing to convince them of its benefits, and this perception is exacerbated by incom-petent workers who may worry about losing their jobs due to a lack of education or training. The adoption of TQM will either succeed or fail, according to trade groups. Therefore, it is assumed that bureaucratic administration fuels opposition to change.
Teamwork may be a solution if values like “working together” and “leaving no one behind” are deeply instilled in the system. Employees will feel as if they are work-ing for one another when a team is cohesive and focused on a single goal. On the other hand, poorly run teams may hurt a group more than not having any at all. The members of the team might develop trust and support for one another under the direction of an excellent team leader. It will be able to support one another and help each other achieve the organization’s goals. Senior leaders’ backing will therefore actively contribute to better patient care in the healthcare sector. Rah-man (2019) claims that top-management support, leadership, cooperation, train-ing, competence development, and organisational culture are characteristics of TQM adoption. As a result, cooperation has to become ingrained in the healthcare system via the formation of the proper culture, ongoing training, and growth.
The kind of training offered to workers would depend on their particular talents,
objectives, needs, and hierarchical position. Managerial cadres may get general leadership training, experts can receive technical training, and leadership cadres and specialists can both receive Total Quality Management training. Specialists may acquire specific training in the use of certain tools or procedures according on their job needs. Business success and service excellence are crucial success cri-teria for the application of TQM in service sectors, according to Talib, Rahman, and Qureshi (2010). Based on expected benefits and CSFs, each company must decide who will get general or customised training.
In order to understand and use TQM, training must be efficient and methodical. It may be done by determining the need for training, creating suitable training programmes, and putting them into action. Employees would get the necessary assistance to advance their skills if they received training. It may be tailored in terms of efficiency-enhancing training goals and by assessing the effectiveness of training activities. Employee interactions and training, according to Ali et al. (2017), may have a good effect on company. The effectiveness of training should be evaluated and assessed by line administrators. As a consequence, it is assumed that ineffective training leads to poor TQM expertise. The bulk of the time, work-ers are the main opponents of change, despite claims like “change is always for the better,” “change is the only constant,” or “change is always resisted.” The TQM initiative could not succeed without complete management backing. Employee participation is crucial to the effectiveness of TQM adoption and management. According to Sadikoglu and Olcay (2014), companies should boost employee in-volvement, devotion, and understanding in order to overcome TQM’s challenges. TQM will suffer considerably if a manager behaves more like a mailman than a “change agent.” In order to achieve TQM, the manager must be responsible and take initiative. One of the most crucial TQM characteristics is the top man-agement’s dedication to employee empowerment since it promotes a solid and long-lasting connection with end users. It will boost sales, earnings, revenues, and customer happiness. Only with caring and empowered employees, pleased and devoted workers, and these goals can be met. Employee empowerment should thus be most successful in overcoming gaps and tying together silos to lessen employee resistance to change. Employees that are open to change will be proac-tive, content, and devoted, which will enable them to concentrate on consumers and adopt a customer-centric mindset. As a result, it is predicted that overcoming change resistance would increase staff empowerment and customer focus.
A simple organisational structure is necessary for Total Quality Management to succeed. The delivery of healthcare services is hampered by the fact that typical healthcare organisations are composite in form and complicated in functioning, with several bureaucratic layers and functional units. Synchronisation is challeng-ing to do in the stated composite structure. In a complex environment, it is chal-lenging to establish Quality Circles (QC), which is a need for Total Quality Manage-ment (TQM) in an organisation. It cannot survive in a complex and sophisticated system, particularly in the lack of leadership commitment and encouragement. Albliwi et al. (2014) claim that among other things, a lack of leadership commit-ment, engagement, communication, training, and proper resources contributed to the TQM catastrophe. The establishment of the QC requires the creation of a steering committee, which also calls for the nomination of QC volunteers and the
identification of senior staff facilitators. The QC suggestions must also be carried out exactly.
The organisation is always changing to improve overall SQ since QC is likely to bring about change through CI. The quality will be improved in order to address service gaps and meet and surpass consumers’ expectations. As a result, customer input must be gathered on a frequent basis. Teams responsible for quality control must often work nonstop to satisfy customers and end users. Consumer loyalty, according to Kassinis and Soteriou (2003), increases sales and lowers future trans-action costs. As a result, QC and CI must be incorporated and act as the “bricks” of TQM’s structure. Therefore, it is predicted that TQM experts would improve Continuous Improvement and the Quality Circle.
The three primary quality-related idea threads of inspection, quality circle, and quality assurance, which gave rise to multiple certifications like ISO 9000, ISO 14000, etc., have come together to form the TQM. According to Carnerud and Backstrom (2019), SQ and end-user satisfaction, process design and control, ISO certification and standards, and process design and control have all been focal points for quality. In 1987, the International Organisation for Standardisation (ISO) proposed seven essential quality management tools. Customer-centricity, effec-tive leadership, staff involvement, process- centricity, ongoing improvement, and evidence-based decision- and relationship-making. It mostly concentrated on managing people and organisational leadership. Sampaio, Saraiva, and Rodrigues (2011) state that the following is the driving force for the adoption of ISO 9000:
A CSF that attests to the successful financial management and quality manage-ment of several organisations. Total Quality Management (TQM), which promoted rigorous procedures to get rid of waste and incompetence, adopted Lean Man-agement (LM) as a key component. There are multiple LM categories with con-flicting purposes and scopes, according to Bhamu and Sangwan (2010). LM looks for things that bring value and gets rid of the ones that don’t. Additionally, it calls for a decrease in unnecessary transportation, inventory, work, overproduction, overprocessing, and flaws. Lean manufacturing processes, according to Choom-lucksanaa, Ongsaranakorn, and Suksabaia (2015), reduced time, expenditure, and non-value-added tasks. LM is more interested in exposing production- process ineptitude than in advocating for a quality system.
Lean and Six Sigma (LSS) integration is important since it focuses on lighting the flow of ideas and materials while Six Sigma processes provide value to changes, claim Antony, Snee, and Hoerl (2017). A similar corporate model is Six Sigma, which aims to provide excellent customer service. Therefore, it is crucial that the healthcare sector invest enough time and energy into understanding the advan-tages and effectiveness of Six Sigma. The urge to implement Six Sigma has led to persistently high hopes for what Six Sigma can accomplish, claim Nakhai and Neves (2009). Six Sigma will probably make it possible for work to advance, grow, and expand in the future, opening up fresh possibilities for a stable future in the industry.
Input from customers, improvements to design and control procedures, as well as
experimental techniques like innovation, originality, and revolution are all stressed by Six Sigma, according to Muoz and Gutierrez (2017). The future of operation management and the service sector lies in the marriage of Lean and Six Sigma. Those who have previous knowledge of one LSS or the other idea encounter a challenge when merging the two, claim Muraliraj et al. (2018). Nevertheless, LSS was introduced to the industry in the first decade of the new century. TQM exper-tise is thus expected to define policies, procedures, processes, and strategy.
The healthcare system is moving steadily in the direction of quality improvement, yet there have been numerous concerns raised about TQM’s efficacy as a tech-nique. The success or failure of TQM must be determined, claim Kim, Kumar, and Murphy (2010); however, this is difficult since TQM is always changing. TQM will surely be effective when particular sets of practises are used.
Acceptance and discussion are both restricted in the healthcare sector. There is a dearth of TQM research in the context of healthcare, claim Alzoubi et al. (2019).It was found that in order to implement transformational change inside an organi-sation, top-level management support, staff training, and growth are essential. It may result in an improvement in an organization’s overall operational effective-ness. Taddese and Osada (2010) claim that TQM primarily affects techno-process innovation via the mediation of working conditions and human resources. To alter management practises and organisational cultures is the ultimate aim of TQM im-plementation in the healthcare sector. The general working qualities of a business, such as job happiness, staff loyalty, retention and dedication, and industry com-petitiveness, are likely to improve with a deeper grasp of TQM. Ansari, Farooqui, and Gattoufi (2018) contend that service businesses should prioritise staff loyalty in order to improve SQ and foster stronger customer interactions.
Factors related to TQM will have an impact on employee loyalty. As workers may increase production and performance, they are an organization’s most import-ant asset. The prosperous company sees its workers as the “prime movers” in achieving achievements as soon as feasible. Quality is an important aspect that has direct implications on employee benefits, customer happiness, and company performance, claim Psomas et al. (2014). Performance improvement should be thoroughly managed by the business since it directly affects the company’s prof-itability. Yee, Yeung, and Cheng (2011) assert that there is a strong connection between service quality, employee and customer satisfaction/loyalty, and a com-pany’s profitability. As a result, it is projected that TQM crucial variables would fuel TQM benefits.
Research Implication
This research sought to understand how technology affected TQM, how people understood TQM practises, how TQM benefited patients and society, and how it may improve business profitability. TQM may be used as a synergistic system implementation technique, resolving both clinical and administrative issues. By supporting efficient healthcare delivery and constant improvement, it may raise patient happiness and loyalty. TQM has gotten a lot of attention across all fields,
including academics, managerial application, and operation management.
Repercussions on the Services Industry
TQM research has a lot of potential in the service sector. According to Ozdal and Oyebamiji (2018), the use of TQM methodologies spans from executive manage-ment to staff satisfaction. It may boost business effectiveness and boost both em-ployee and customer satisfaction. TQM Planning well and receiving funding are essential, but poor management might jeopardise TQM. Sampaio, Saraiva, and Domingues (2012) assert that it is important to look at a variety of business re-quirements, such as leadership dedication, resource accessibility, communication, and training and development.
Applications for Administration
TQM will provide good management opportunities for reducing waste, enhancing product and SQ, and boosting sales and profit. To overcome change resistance, it may be done through developing a TQM culture, offering leadership support, empowering people, and mending the gaps between employees and manage-ment. Rahman (2019) asserts that unity, employee mentorship, and leadership commitment are characteristics of the best TQM implementation. As soon as they are satisfied and dependable, employees will value TQM.
Software for Operational Management
All kinds of sectors may undergo change as a consequence of TQM, and this transformation will help society by boosting customer happiness, productivity, cutting waste, reducing defects, lowering costs, increasing revenues, and increas-ing profitability. By boosting productivity, lowering operational expenses, and improving customer happiness, staff loyalty, and employee engagement, it will increase the company’s competitive position. Implementing TQM is linked to en-hanced organisational performance, claims Joiner (2007). All parties involved will get a higher return as a result, adding value to the situation. When implementing TQM by engaging labour unions, industry must move carefully since any dispute might make or destroy TQM.
The current structure is quite advantageous, which will result in TQM advantages for achievers. Bureaucracy is the main obstacle to adopting TQM in the healthcare industry since healthcare settings are often departmentalized with a large num-ber of units, sub-units, and subsystems that are linked by a web of management controls. This calls for several “command and control” systems and degrees of hierarchy. TQM is incompatible with a management style that is so bureaucratic. Candido and Santos (2011) claim that even if there is no empirical support, the
sheer cost of adopting TQM may deter many companies from doing so. Lack of leadership commitment or insufficient cooperation, inefficient training and pro-gression, a lack of employee empowerment, a lack of processes and procedures, and even the absence of QC and CI are all major barriers to TQM adoption.
Conclusion
The essential components of TQM, according to the conclusions, would result in advantages like increased customer engagement and patriotism due to the com-mitment and loyalty of employees, waste reduction via environmental respon-sibility, and growth in revenue, profitability, and shareholder value. Conclusions also show that technology-enabled healthcare TQM services will boost client hap-piness, retention, good word of mouth, revenue, and profitability. Ansari (2020) asserts that SQ enhances customer loyalty and happiness, boosts employee pride and effort, and promotes the practise of repeat purchases.
To get to this point, one must be open to change, eager to learn more, ready to participate in establishing structures like QC and CI, and knowledgeable enough to reap the advantages of TQM. The current study therefore affirms that TQM deployment in healthcare would increase performance when done so under the right circumstances, with dedicated leadership, a quality circle established, a help-ful infrastructure, and a mindset of continuous quality improvement. According to the current TQM framework, healthcare providers may identify practical TQM implementation aspects by removing obstacles to TQM and concentrating on maximising its advantages. Healthcare managers may come up with more effec-tive plans to overcome some of the biggest challenges and achieve a favourable, conducive condition from which they can reap the “desired” advantages if they are armed with a clear-cut TQM framework. Lack of understanding of Total Qual-ity Management may be a research constraint. However, only a tiny sample of respondents—who may not accurately reflect the community at large—were sub-jected to in-depth interviews. Future study that uses structural equation model-ling and empirical validation is therefore needed to evaluate the potential impact of Lean Manufacturing and Six Sigma integrated as LSS on the healthcare sector.
References
Ali, F., Jain, R., Ali, L. and Munir, K., 2017. The Effects of Quality Practices on the Performance Measurement of Business Management. Journal of Advanced Management Science, 5(6), pp.440-
444. DOI: 10.18178/joams.5.6.440-444.
Ali, K.A.M. and Alolayyan, M.N., 2013. The impact of total quality management (TQM) on the hospital’s performance: an empirical research. International Journal Services and Operations Man-agement, 15(4), pp.482-506. DOI: 10.1504/IJSOM.2013.054904.
Alzoubi, M.M., Hayati, K.S., Rosliza, A.M., Ahmad, A.A. and Al-Hamdan, Z.M., 2019. Total qual-ity management in the health-care context: integrating the literature and directing future research. Risk Management and Healthcare Policy, 12, pp.167-177. DOI: 10.2147/RMHP.S197038.
Ansari, M.S.A., 2020. Extended Service-Profit Chain for Telecom Service Industry in Oman: An
Empirical Validation. Sustainable Futures, 2, 10pp. DOI: 10.1016/j.sftr.2020.100032. Ansari, M.S.A., Farooquie, J.A. and Gattoufi, S.M., 2018. Emotional Intelligence and Extended Service Profit Chain in Telecom Emotional Intelligence and Extended Service Profit Chain in Telecom. International Business Research, 11(3), pp.133-148. DOI: 10.5539/ibr.v11n3p133.
Antony, J., Snee, R. and Hoerl, R., 2017. Lean Six Sigma: yesterday, today and tomorrow. International Journal of Quality & Reliability Management, 34(7), pp.1073-1093. DOI: 10.1108/ IJQRM-03-2016-0035.
Balasubramanian, M., 2016. Total Quality Management in the Healthcare Industry, Challeng-es, Barriers and Implementation Developing a Framework for TQM Implementation in a Healthcare Setup. Science Journal of Public Health, 4(4), pp.271-278.
Bhamu, J. and Sangwan, K.S., 2010. Lean manufacturing: literature review and research issues. International Journal of Operations & Production Management, 34(7), pp.876-940. DOI: 10.1108/ IJOPM-08-2012-0315.
Cameron, R. and Azorin, J.F.M., 2011. The acceptance of mixed methods in business and management research. International Journal of Organizational Analysis, 19(3), pp.256-271. DOI: 10.1108/19348831111149204.
Candido, C.J.F. and Santos, S.P., 2011. Is TQM more difficult to implement than oth-er transformational strategies. Total Quality Management journal, 22(11), pp.1139-1164. DOI: 10.1080/14783363.2011.625185.
Carnerud, D. and Bäckström, I., 2019. Four decades of research on quality: summarizing, trendspotting and looking ahead. Total Quality Management & Business Excellence,
32(9-10), pp.1023-1045. DOI: 10.1080/14783363.2019.1655397.
Choomlucksanaa, J., Ongsaranakorna, M. and Suksabaia, P., 2015. Improving the productivity of sheet metal stamping subassembly area using the application of lean manufacturing principles. Procedia Manufacturing, 2, pp.102-107. DOI: 10.1016/j.promfg.2015.07.090.
Creswell, J.W., 1998. Qualitative inquiry and research design: Choosing among five traditions.
Thousand Oaks, CA: Sage.
Dahlgaard, J.J., Pettersen, J. and Park, S.M.D., 2011. Quality and lean health care: A system for assessing and improving the health of healthcare organisations. Total Quality Management & Business Excellence, 22(6), pp.673- 689. DOI: 10.1080/14783363.2011.580651.
Dale, B.G., Wiele, T.V.D. and Iwaarden, J.V., 2013. Managing quality. 5th ed. Blackwell Pub-lishing.
Deming, E., 1986. Out of the crisis. Cambridge, Mass.: Massachusetts Institute of Technology, Centre for Advanced Engineering Study.
Dénes, R.V., Kecskés, J., Koltai, T. and Dénes, Z., 2017. The Application of Data Envelopment Analysis in Healthcare Performance Evaluation of Rehabilitation Departments in Hungary. Quality Innovation Prosperity, 21(3), pp.127-142. DOI: 10.12776/qip.v21i3.920.
Deros, B.M., Yusof, S.M. and Salleh, A.M., 2006. Perceptions and practices of critical suc-cess factors in benchmarking implementation in Malaysian automotive manufacturing companies. Journal of Quality Measurement and Analysis, 2(1), pp.45-61.
Hackman, J. R., and Wageman, R., 1995. Total quality management: Empirical, conceptual, and practical issues. Administrative Science Quarterly, 40,(2), pp.309-342. DOI: 10.2307/2393640.
Hassan, M., Mukhtar, A., Qureshi, S.U. and Sharif, S., 2012. Impact of TQM Practices on Firm’s.
Performance of Pakistan’s Manufacturing Organizations, 2(10), pp.232-259.
Ishikawa, K., 1985. What Is Total Quality Control? The Japanese Way. Englewood Cliffs, N.J.: Prentice-Hall.
Izogo, E.E. and Ogba, I.E., 2015. Service quality, customer satisfaction and loyalty in auto-mobile repair services sector. International Journal of Quality & Reliability Management, 32(3), pp.250-269. DOI: 10.1108/IJQRM-05-2013- 0075.
Joiner, T.A., 2007. Total quality management and performance. The role of organization sup-port and co-worker support. International Journal of Quality & Reliability Management, 24(6), pp.617-627. DOI: 10.1108/02656710710757808.
Juran, M.J., 1989. Juran’s Quality Handbook. McGraw-Hill Companies.
Kajihara, C., Munechika, M., Kaneko, M., Sano, M. and Jin, H., 2016. A Matrix of the Functions and Organizations that Ensure Continued Healthcare Services in a Disaster. Quality Innovation Prosperity, 20(2), pp.145-156. DOI: 10.12776/qip.v20i2.747.
Kassinis, G.I., and Soteriou, A.C., 2003. Greening the service profit chain. The impact of en-vironmental management practices. Production and operation management, 12(3), pp.386- 403. DOI: 1059-1478/03/1203/386$1.25.
Khan, M.N., Malik, S.A. and Janjua, S.Y., 2008. Total Quality Management practices and work-re-lated outcomes, A case study of higher education institutions in Pakistan. International Journal of Quality & Reliability Management, 36(6), pp.864-874. DOI: 10.1108/IJQRM-04-2018-0097.
Kim, D.Y., Kumar, V. and Murphy, S.A., 2010. European Foundation for Quality Management Business Excellence Model: An integrative review and research agenda. International Journal of Quality & Reliability Management, 27(6), pp.684-701. DOI: 10.1108/02656711011054551.
Kumar, V., Sharma, R.R.K., Lai, K.K. and Chang, Y.H., 2018. Mapping the TQM, Implementation, An empirical investigation of the cultural dimensions with different strategic orientation in Indian firms. Benchmarking: An International Journal, 25(8), pp.3081-3116. DOI: 10.1108/BIJ-06-2017-0150.
Morse, J.M., 1994. Designing funded qualitative research. In: N.K. Denzin and
Mosadeghrad, A.M., 2013. Obstacles to TQM success in health care systems. International Journal of Health Care Quality Assurance, 26(2), pp.147-173. DOI: 10.1108/09526861311297352.
Muñoz, C.A. and Gutierrez, L.J., 2017. Six Sigma and organizational ambidexterity: a system-atic review and conceptual framework. International Journal of Lean Six Sigma, 8(4), pp.436-456. DOI: 10.1108/IJLSS-08-2016- 0040.
Muraliraj, J., Zailani, S., Kuppusamy, S. and Santha, C., 2018. Annotated methodological review of Lean Six Sigma. International Journal of Lean Six Sigma, 9(1), pp.2-49. DOI: 10.1108/ IJLSS-04-2017-0028.
Nakhai, B. and Neves, J.S., 2009. The challenges of six sigma in improving service
Parasuraman. A. and Grewal, D., 2000. The impact of Technology on the Quality-Value- Loyal-ty Chain: A research agenda. Journal of the Academy of Marketing Science, 28, pp.168-
174. DOI: 10.1177/0092070300281015.
Parasuraman. A., Zeithaml, V.A. and Berry, L.L., 1985. A conceptual model of service quality and its implications for future research. Journal of marketing, 49(3), pp.41-50.
Prajogoa, D.I. and Hong, S.W., 2008. The effect of TQM performance in R&D environments: A perspective from South Korean firms. Technovation, 28(12), pp.855-863. DOI: 10.1016/j.techno-vation.2008.06.001.
Psomas, E., Vouzas, F. and Kafetzopoulos, D., 2014. Quality management benefits through the “soft” and “hard” aspect of TQM in food companies. The TQM Journal, 26(5), pp.431- 444.
DOI: 10.1108/TQM-02-2013-0017.
Rahman, M., 2019. A Literature Review Based Analysis of Total Quality Management (TQM) Implementation towards Quality Improvement in Bangladeshi Hospitals. International Journal of Progressive Sciences and Technologies (IJPSAT), 17(2), pp.11-16.
Rust, T.R., Zahorik, A.J. and Keiningham, T.L., 1995. Return on Quality (ROC): Making Service Quality Financially Accountable. Journal of Marketing, 59(2), pp. 58-70. DOI: 10.2307/1252073.
Sadikoglu, E. and Olcay, H., 2014. The Effects of Total Quality Management Practices on Performance and the Reasons of and the Barriers to TQM Practices in Turkey. Advances in Decision Sciences, 2014, 17p. DOI: 10.1155/2014/537605.
Sampaio, P., Saraiva, P. and Domingues, P., 2012. Management systems: integration or addition?. International Journal of Quality & Reliability Management, 29(4), pp.402-424. DOI: 10.1108/02656711211224857.
Sampaio, P., Saraiva, P. and Rodrigues, A.G., 2011. The economic impact of quality man-agement systems in Portuguese certified companies’ Empirical evidence. International Journal of Quality & Reliability Management, 28(9), pp.929-950. DOI: 10.1108/02656711111172522.
Sila, I. and Ebrahimpour, M., 2002. An investigation of the total quality management survey-based research published between 1989 and 2000. International Journal of Quality & Reliability Management, 19(7), pp.902-970. DOI: 10.1108/02656710210434801.
Slimák, I. and Zgodavova, K., 2011. Focus on Succes. Quality Innovation Prosperity, 15(1), pp.1-4. DOI: 10.12776/qip.v15i1.36.
Taddese, F. and Osada, H., 2010. Process Techno - Innovation Using TQM in Developing Countrie, Empirical Study of Deming Prize Winners. Journal of Technology and Management Inno-vation, 5(2), pp.46-65. DOI: 10.4067/S0718- 27242010000200005.
Y.S. Lincoln, eds. Handbook of qualitative research. Thousand Oaks, CA: Sage. pp.220-235.
Yee, R.W.Y., Yeung, A.C.L. and Cheng, C.E.C., 2011. An empirical Analysis in high contact ser-vice industries. International Journal of Production Economics, 130(2), pp.236-245. DOI: 10.1016/j. ijpe.2011.01.001.
Yusof, S.M. and Aspinwall, E., 2001. Case studies on the implementation of TQM in the UK automotive SMEs. International Journal of Quality & Reliability Management, 18(7), pp.722- 743. DOI: 10.1108/02656710110396058.
Zgodavova, K. and Colesca, S.E., 2007. Quality Management Principles – An Approach In Healthcare Institutions. Management and Marketing Journal, 5(1), pp.31-38.
Get an email when we publish new research and open calls for chapters.
Create a free account